Updates on the Latest News & Research Regarding your Health.
Trending Articles

Anaphylaxis Risk Analysis via Skin Testing with Covid-19 Vaccines Vaccination has been found to be effective in reducing the risks of infection of severe acute respiratory syndrome coronavirus and severe coronavirus disease 2019 (COVID-19) outcomes. In the United States, Pfizer-BioNTech and Moderna COVID-19 vaccines (aka the messenger RNA [mRNA] vaccines) have been used safely for these purposes. 1 , 2 PATIENT HISTORY OF ANAPHYLAXIS First post-market reports on the use of these vaccines describe 4.7 cases of anaphylaxis per million doses of Pfizer vaccine 3 and 2.5 cases per million Moderna doses given. 4 These early reports also describe 43.8 cases of non-anaphylactic allergic reactions per million Pfizer doses given. Among individuals who experienced anaphylaxis to the Pfizer vaccine, 81% had a documented history of allergies triggered by drugs, vaccines, medical products, foods or insect stings, and 33% of these individuals experienced anaphylaxis in the past. Similarly, 90% of individuals with a history of anaphylaxis to the Moderna vaccine had a documented history of allergic reactions, and 50% of these individuals experienced anaphylaxis in the past. POLYETHYLENE GLYCOL IN mRNA VACCINES The presumed causes of allergic reactions are the different polyethylene glycols (PEGs) in the mRNA vaccines. Although PEG allergy is rare, PEG has been found to cause anaphylaxis. 5 Moreover, skin testing of PEGs of differing molecular weights has been found to be effective in confirming anaphylaxis to PEGs in patients with a documented history of anaphylaxis to PEG. 6 Nevertheless, in a cohort of 8 individuals with allergic reactions to the first dosage of an mRNA vaccine, PEG skin testing result was found to be negative. 7 VACCINE PARAMETERS The 2012 vaccine practice parameters published by the American Academy of Allergy, Asthma, and Immunology (AAAAI), recommend that individuals with suspected anaphylaxis to a particular vaccine receive skin testing with that vaccine to evaluate their risk of anaphylaxis. 8 Because the mRNA vaccines contain components other than PEG that may cause allergic reactions, the AAAAI recommendations for evaluating risk of anaphylaxis to vaccines are appropriate for the mRNA vaccines as well. In fact, Greenhawt et. al. 9 recently suggested using the 2012 parameters for patients with a previously documented allergy to one of the mRNA vaccines. 9 Many of our patients who have experienced anaphylaxis express hesitancy toward receiving vaccines, owing to fears of anaphylaxis, and continue to delay their COVID-19 vaccination. To meet this demand, we offered skin testing with mRNA vaccines for our patients who requested evaluation of their risk of anaphylaxis. INITIAL TESTING In this communication, we will describe our first 30 patients (female, n = 27; male, n = 3) who had skin testing with the mRNA vaccines. The patients were either self-referred or referred to us by other physicians. All patients had a self-reported history of anaphylaxis to a variety of substances, including foods, venoms, drugs, environmental, flu vaccine, unknown sources or the first dosage of a COVID-19 mRNA vaccine. The risks and benefits of skin testing were discussed with the patients, and consent forms were accordingly signed. The patients were probed for self-reported reactions to PEG-containing products (ie, toothpaste and colonoscopy preparation). Ages of the patients ranged from 27 to 80 years. Of the patients, 2 had a history of COVID-19 confirmed by polymerase chain reaction testing. Disclosures: The authors have no conflicts of interest to report. Funding: The authors have no funding sources to report. https://doi.org/10.1016/j.anai.2021.09.021 ABOUT THE TEST Skin testing occurred from January 22, 2021, to March 25, 2021. Remnants of the mRNA vaccines were collected on the morning of testing from the Johnson City Medical Center in coordination with the Tennessee Department of Health and used for skin testing within 6 hours from opening of the vials. The patients were advised to refrain from using antihistamines and oral glucocorticoids starting 3 days before the testing. Skin testing was performed on the ventral forearms of the patients using the protocol recommended by the AAAI with modifications to increase safety. Testing began with stan- dard histamine and normal saline applied by prick technique and by intradermal injection of 0.05 mL of each as positive and negative con- trols, respectively. Next, a 1:10 dilution with normal saline of the Pfizer or Moderna vaccine was applied by prick technique. After 20 minutes, wheal sizes were measured and recorded. Whenever the result was negative, every 20 minutes a dosage of 0.05 mL of diluted vaccine was applied intradermally, starting with a 1:1000 dilution, then a 1:100 dilution, and finally a 1:10 dilution. After recording the final wheal size, pictures of the skin tests were taken, the patients were observed for an additional 30 minutes, and they were requested to submit pictures of their skin test at 4 to 6 hours after testing to evaluate late-phase reactions and at 24 hours after testing to evaluate delayed reactions. Afterward, the patients were evaluated by direct interviews for their reaction to subsequent vaccination. RESULTS The results are presented in Table 1 . There were 5 patients who had positive immediate skin reactions at doses ranging from 1:100 to 1:10 dilution of an mRNA vaccine. Of these patients, 1 had an anaphylactic reaction during skin testing of 1:100 dilution of the Moderna vaccine. These 5 patients also had positive late-phase reactions. There were 6 patients who had late-phase reactions without immediate reactions. Unfortunately, most patients did not comply with our request to submit pictures from delayed reaction. Patients with positive immediate reactions were recommended to receive the Janssen COVID-19 vaccine. Patients with negative immediate reactions (n = 25) were recommended to receive their choice of COVID-19 vac- cine. None of the patients with negative skin test result to an mRNA vaccine who were subsequently vaccinated to COVID-19 (n = 19, con- firmed through records in the Tennessee Immunization Information System) have had any allergic reaction to vaccination. After our risk assessment, 66% of the patients went on to receive full COVID-19 immunization.

Take a Look: Facts and fiction behind popular allergy myths. AND: How you can protect yourself— all year long. We are about to embark upon the fall allergy season in full swing. It is important to know the dos and don’ts regarding allergies and what is actually accurate information surrounding them. After reading an article entitled “8 common myths about allergies,” written by Alistair Gardiner, we wanted to share useful information to help you prepare for not only fall allergy season, but all year long as well. ALL ABOUT POLLEN A lot of people dread to see flowers bloom in the spring, but according to research, the trees in that season, grasses in the summer, weeds in the fall, and mold spores, which can occur anytime, but primarily in the fall and winter, are the predominant culprits of allergy producing symptoms. This can produce allergic rhinitis, known to many as hay fever, which consists of sneezing, nasal drainage, chronic sinusitis, itchy, watery eyes, as well as asthma with cough and wheezing. During the allergy seasons individuals with allergy syndrome can feel more tired and irritable. This is because these particular pollens are airborne and are more likely to be inhaled through the nose and cause these symptoms rather than flower pollens, which appear to be larger and have a sticker texture allowing them to adhere to insects and not be as prevalent in the air. The pollens of trees, grasses, weeds, and mold spores cause many symptoms that we see daily in our clinics. We recommend allergy immunotherapy, also known as allergy injections, for sick patients with multiple symptoms which test positive for these allergens either by skin or blood test. A new treatment that has been introduced and effective in helping allergy suffers are immunological modifiers known as biologicals. PROGRESSION OF ALLERGY Another misconception is that if one never developed allergies as a child, one won’t every have problems with them in the future. According to Dr. Neeta Ogden of the ACAAI, age is not a factor for when allergies can occur. “In fact, more than half of adults with food allergies tend to develop them during adulthood” (Gardiner, 2021). More and more adults in their early adulthood (20s and 30s) are beginning to develop allergy syndrome, according to an allergist, Edward David, III, MD (Gardiner, 2021). This is a very common finding in our practice, and many are indeed shocked to not only develop environmental and food allergies at this later age, but sometimes life-threatening ones as well. Next, we look at the question, do allergies last forever? Many think they never go away. For some, that may be the case. Some have symptoms that come and go over times, and some do eventually develop an immunity to them as they age or complete their treatment plan. Typically symptoms of allergy change from acute, to subacute, to chronic with fatigue their primary complaint. Where there are environmental allergies like ragweed pollen in the fall, there are almost always food allergies because of the cross reactions between the two. So, the ragweed pollen allergen cross react with gourd plants and while eating those and exposure in weeds can increase symptoms. Avoiding these reactive foods helps decrease allergy or other symptoms that they may cause, and patients may eventually be able to tolerate them with more ease. Mayo Clinic states that about 60-80% of children with milk and/or egg allergies may be able to eat these foods without problems by the time they reach sixteen years of age (Gardiner, 2021). However, there are occasions where this is not possible despite treatment and/or avoidance. It appears that certain tree nuts and shellfish may pose a different stance, and these may never be able to be consumed without problems. PET ALLERGIES Next, we will discuss one of the most sensitive topics in allergy, and that is pets. These beloved creatures can cause an array of problems for their owners if they are allergic to them. What is one specifically allergic to regarding pets? The most common misconception is the fur itself. Instead, it has nothing to do with the fur at all. It is the dander, which contains all sorts of allergens, such as saliva, skin flakes, urine, and a multitude of other pollens they pick up when they are outside (Gardiner, 2021). Also, many think there are hypoallergenic dogs or cats, but according to the AAAI, that is not true (Gardiner, 2021). Certain pets may cause more allergy symptoms in certain people than others, but this is not related to its fur or certain breeds specifically. If one would still like their furry friends around, some things to do are to groom them regularly and try to keep them out of one’s bedding to decrease exposure. FOOD ALLERGY The next topic at hand is finding the difference between food allergies and food intolerances. Are they the same? The answer is no. Food allergies illicit an “adverse immune response to certain proteins, which lead to dermatologic, respiratory, gastrointestinal, cardiovascular, and/or neurologic symptoms” (Gardiner, 2021). As mentioned earlier, some allergies can trigger a near fatal experience, also known as anaphylaxis, especially certain foods for certain individuals. Food intolerances do NOT provoke an immune response but involve reaction due to toxicity or lack of some enzymes to process foods like lactase (associated with lactose intolerance). To manage immunological reactions of food we recommend cooking or fermenting most foods since it tends to denature most proteins, making reactive foods more tolerable. In addition to avoidance of reactive foods, adding probiotics from fermented food, and adhering to a paleo diet may help to decrease symptoms and strengthen the immune system. This is an approach also used in our clinics with success. Last, but not least, let’s discuss peanuts. Many think this food causes the most severe reactions of all foods. It does for some, but not for others. This is all contingent on one’s immune system as to how it responds. “According to Food Allergy Research and Education, there are actually eight foods identified as causing the most serous reactions for people in the U.S.” (Gardiner, 2021). They are crustacean shellfish, eggs, peanuts, milk, wheat, tree nuts, soy, and fish (Gardiner, 2021). It is important to understand myths regarding allergies because it can help one to know how to better protect oneself against symptomatology and/or potential life-threatening experiences.

CDC's ACIP Expands on Precautions and Contraindications for Pfizer Vaccine New Updated Information as of January 6, 2021. https://www.cdc.gov/vaccines/covid-19/info-by-product/clinical-considerations.html What to know: “Severe allergic reaction (e.g., anaphylaxis) to any component of the Pfizer-BioNTech COVID-19 vaccine is a contraindication to vaccination listed in the prescribing information. Anaphylactic reactions in persons outside of clinical trials have been reported. While these reports are further investigated, CDC considers a history of severe allergic reaction (e.g., anaphylaxis) to any other vaccine or injectable therapy (e.g., intramuscular, intravenous, or subcutaneous) as a precaution but not a contraindication to vaccination. In persons who report a history of anaphylaxis to another vaccine (i.e., any other vaccine besides the Pfizer-BioNTech COVID-19 vaccine) or injectable therapy, a risk assessment should be conducted to determine type of reaction and certainty of information. For example, whether the medication was administered by injection or another route or whether the reaction constituted a severe allergic reaction (e.g., required use of epinephrine [EpiPen®, etc.], resulted in hospitalization). These persons may still receive vaccination, but they should be counseled about the unknown risks of developing a severe allergic reaction and balance these risks against the benefits of vaccination. A history of mild allergic reaction to a vaccine or injectable therapy, such as urticaria alone without signs or symptoms of anaphylaxis, is not a contraindication or precaution to Pfizer-BioNTech COVID-19 vaccination. In addition, allergic reactions (including severe allergic reactions) not related to vaccines or injectable therapies (e.g., food, pet, venom, environmental, or latex allergies; oral medications [including the oral equivalents of injectable medications]) are not a contraindication or precaution to vaccination with Pfizer-BioNTech COVID-19 vaccine.” Additional discussion about clinical considerations for use of the vaccine can be found here . Allergists need to know that the CDC/ACIP/FDA and NIAID are aware of the reactions that have occurred and are actively working, along with leadership of the AAAAI, to determine the cause for these reactions, and developing protocols to help you deal with them. Added Precautions The CDC has also issued guidelines on precautions and management of anaphylaxis to sites that administer the vaccines. Recommendations are to avoid any other vaccinations for 14 days before or after the SARS-CoV-2 vaccine, but if you have had another vaccine within that 14 day window, don’t wait to get this vaccine. Recommendations are to defer vaccination for 90 days after receiving convalescent plasma or monoclonal antibody treatment for COVID-19. About the Moderna Vaccine: This vaccine has been granted an EUA and approval from the CDC/ACIP . Results from the clinical trials are very similar in efficacy and safety compared to the Pfizer vaccine. The FDA Briefing Document can be found here . This document presents both interim analysis using a data cutoff of November 7, with a median follow-up of 7 weeks post-dose one, and the final scheduled analysis from a data cutoff of November 21, with a median follow-up >2 months post-dose two. This summary covers the final scheduled analysis. Safety: The most common adverse reactions: injection site pain (91.6%), fatigue (68.5%), muscle pain (59.6%), joint pain (44.8%), chills (43.4%), fever (14.8%). Most of these were mild to moderate, began on day 1-2 and lasted 2 days. A small number of participants reported systemic reactions longer than 7 days, but there was no difference between vaccinated and placebo groups. Lymphadenopathy (axillary) was reported in 21.4% of vaccine recipients <65 years of age, and 12.4% in those >65 years of age, compared to 7.5% and 5.8% in placebo in those age groups respectively. Severe adverse reactions occurred in 0.2% to 9.7% of participants, and were more frequent after the second dose and less common in those 65 years of age and older. Hypersensitivity adverse events were slightly greater in the vaccine group (1.5%) compared to the placebo group (1.1%). There were no anaphylactic or severe hypersensitivity reactions. This vaccine also contains PEG in the lipid capsule. Serious adverse events were low (1.0%) without meaningful imbalances between study arms. Other than the differences in the age groups and reactogenic reactions, there were no safety differences with respect to race, ethnicity, gender or pre-existing conditions. Efficiency: Vaccine efficacy was 94.1% (95% CI 89.3%, 96.8%) with 11 cases of COVID-19 in the vaccine group and 185 cases in the placebo group. Unlike the interim data, the vaccine efficacy when stratified by age group was 95.6% (95% CI 90.6%, 97.9%) for participants 18 to <65 years of age and 86.4% (95% CI 61.4%, 95.5%) for participants 65 years of age or older. Other than the age group difference, there were no vaccine efficacy differences based on race, ethnicity, gender or medical comorbidities associated with high risk for severe COVID-19. Vaccine efficacy against severe COVID-19: 30 cases in the placebo group, 0 in the vaccine group. Vaccine efficacy after the first dose was 80.2% (95% CI, 55.2%, 92.5%) in the 2,000+ patients who only received one dose, but these patients were only followed for 28 days. *Efficacy against asymptomatic infection: preliminary data only, NP swabs were collected pre-dose one and pre-dose two. Number of positive swabs pre-dose two in negative baseline participants was 14 in the vaccine group and 38 in the placebo group, suggesting that some asymptomatic infections may be prevented with just the first dose.

Fermented foods can ease the symptoms you feel in your gut. Here's why: The symptoms you feel in your gut are caused by your unbalanced immune system producing too much inflammation. In order to balance your immunity and reduce inflammation in your gut, it is important to restore balance to the helpful bacteria that live in your gut. Those helpful bacteria come in hundreds of different types and have many functions including helping you digest, unlocking nutrients in foods, and maintaining a healthy immune system. 1 Restoring balance to the huge ecosystem of helpful bacteria in your gut requires eating helpful bacteria. 2,3,4 The best source of those helpful bacteria is from fermented foods such as sauerkraut, yogurt, or kombucha. These foods are such a good source of helpful bacteria because the fermentation process allows for a diverse collection of helpful bacteria to multiply and grow on the foods. When we eat these fermented foods, those helpful bacteria then begin living in our gut where they help maintain a healthy immune system. Where can I buy Fermented Foods? The best place to get your fermented foods is from your own home. Eating food that you ferment yourself will ensure that you are getting the largest diversity of helpful bacteria possible. If you do choose to ferment your own foods, do not can your fermented foods. The canning process kills all the helpful bacteria in your fermented foods. Fortunately, there are some fermented food products available at the grocery store. In the grocery store, look for fermented products that are unpasteurized, that use a SCOBY (symbiotic culture of bacteria and yeast) and/or that list many different types of helpful bacteria in the product. A few examples of these products are provided at the end of this packet. Alternatively, ask your local farmers about any fermented products they may sell. Fermented Foods at Home vs Mass-Produced Fermentation Traditionally, foods get fermented when we allow helpful bacteria to break down food in a controlled environment. This fermentation process allows a diverse collection of helpful bacteria to grow on the food. When we eat these foods, those helpful bacteria begin living in our gut where they help us digest foods, unlock nutrients in foods, and maintain a healthy immune system. The process of industrially producing fermented foods reduces the diversity and number of helpful bacteria in those foods. In this industrialized process, foods are first fermented then heated up to kill all the helpful bacteria in the food (aka pasteurized) and then packaged. These steps are taken to increase shelf life. Sometimes after heating, the foods are injected with a selection of a couple helpful bacteria for health benefits. However, using only a couple of different types of helpful bacteria means those foods have less diversity of helpful bacteria than traditionally fermented foods. This reduction in diversity makes industrially produced fermented foods less effective in restoring balance to the helpful bacteria in your gut and, ultimately, less effective in easing your gut symptoms. Fermented products at the grocery store that are unpasteurized, that do not use preservatives, that use a SCOBY, and/or that list the many helpful bacteria in the product are more likely to contain a large diversity of helpful bacteria. Even better, foods fermented at home or by your local farmers contain a huge diversity of helpful bacteria. Food Allergy and Fermentation In addition to helping maintain a healthy immune system, eating fermented foods can also reduce your risk of eating something that gives you an allergic reaction. When most foods ferment, the part of the food that causes allergic reactions is broken down. 5 , 6 So, you may be allergic to milk or cabbage, but you still may be able to eat yogurt or sauerkraut without experiencing allergic symptoms. Probiotic Supplements and food options can be found at your local grocery store. Probiotic supplements contain a selection of a few types of helpful bacteria. While these pills can be useful in certain situations, even the best probiotic supplements only contain a few different types of helpful bacteria while a healthy human gut contains hundreds of types of helpful bacteria. Due to this lack of diversity in probiotic pills, eating fermented foods containing a large diversity of helpful bacteria can be more effective in restoring the balance of helpful bacteria in your gut. We've assembled a list of ways that can help you identify what to avoid and what to buy. Look for a list of helpful bacteria. If allergic to dairy, try milk kefir alternatives. Look for Kombucha that utilizes SCOBY. Look for foods that are unpasteurized. Check for ingredients you may be allergic to such as wheat proteins. Check that there are no preservatives in the ingredients list. Examples of Common Fermented Foods Saurekraut Kimchi Sour Pickles Olives Capers Dilly Beans Water Kefir (aka Tibicos) Kombucha Yogurt Milk Kefir Almond Milk Kefir Creme Fraiche Buttermilk Farmstead cheese Miso Tempeh Fish Sauce Soy Sauce Fermented Black Bean *Sour pickles are different from regular pickles. Regular pickles are made by adding vinegar to the vegetable, also known as pickling. This process does not allow helpful bacteria to grow so eating ‘regular’ pickles, is not helpful in restoring balance to your gut bacteria. Sour pickles are made by way of fermenting the vegetable in a similar manner to the sauerkraut making process. Almost any vegetable can be made into a sour pickle including cucumbers, carrots, green beans, okra, cauliflower, radishes, peppers, etc. 1 Goto, Yoshiyuki, and Hiroshi Kiyono. “Epithelial Barrier: an Interface for the Cross‐Communication between Gut Flora and Immune System.” Wiley Online Library, John Wiley & Sons, Ltd, 15 Dec. 2011, onlinelibrary.wiley.com/doi/abs/10.1111/j.1600-065X.2011.01078.x. 2 Veiga, Patrick, et al. “Changes of the Human Gut Microbiome Induced by a Fermented Milk Product.” Nature News, Nature Publishing Group, 11 Sept. 2014, www.nature.com/articles/srep06328. 3 Derrien, Muriel, and Johan E.T. van Hylckama Vlieg. “Fate, Activity, and Impact of Ingested Bacteria within the Human Gut Microbiota.” Trends in Microbiology, Elsevier Current Trends, 1 Apr. 2015, www.sciencedirect.com/science/article/pii/S0966842X15000566. 4 Oozeer, Raish, et al. “Survival of Lactobacillus Casei in the Human Digestive Tract after Consumption of Fermented Milk.” Applied and Environmental Microbiology, American Society for Microbiology, 1 Aug. 2006, aem.asm.org/content/72/8/5615.short El-Ghaish, Shady, et al. “Potential Use of Lactic Acid Bacteria for Reduction of Allergenicity and for Longer Conservation of Fermented Foods.” Trends in Food Science & Technology, Elsevier, 14 May 2011, www.sciencedirect.com/science/article/abs/pii/S0924224411000926. Shi, Jing, et al. “Effects of Fermentation by Lactobacillus Casei on the Antigenicity and Allergenicity of Four Bovine Milk Proteins.” International Dairy Journal, Elsevier, 5 Nov. 2013, www.sciencedirect.com/science/article/abs/pii/S0958694613002616

No Evidence Suggests Asthma puts patients at higher risk for COVID-19 Covid-19 pandemic frightens a lot of people and traumatically disrupted our social lives. Since virus SARS-COV-2 (the virus which cause COVID-19 syndrome) may attack the lungs there is obvious concern for patients with chronic respiratory diseases including asthma. Initial information about risk of severe disease from China implied that the patients with asthma are more likely to suffer from severe infection and death from this syndrome. It is very important now to recognize that currently there is no evidence implying asthma in the United States (studies in New York and Atlanta) and most recent large studies from England, that patients with asthma are at a higher risk of dying when attacked by the virus. "Recent loss of smell and taste was recognized as symptoms of COVID-19 infection." Though this may not be true for patients with COPD which differ substantially from allergic asthma. Please remember that we are in continuous process of acquiring this information and this current point of view may change in the future. It is critical if you have asthma and allergy that you protect yourself against exacerbation as this potentially puts you at higher risk from acquiring COVID-19. Therefore it is appropriate to continue all your current medications prescribed by your physician for controlling your symptoms including inhaled steroids and biologicals as Omalizumab, Mepolizumab, Reslizumab, Benralizumab and Dupilmab. It is also interesting to note that allergy immunotherapy seems to restore the production of interferon which is one of the main antiviral human responses thus may have effect on viral infections in allergy patients (studies from John Hopkins). Recently loss of smell and taste was recognized as symptoms of covid infection. As you know these symptoms are quiet common for patients with allergy specially those which suffer with polyps in the nose. Thus proper diagnosis of Covid infection needs to take proper medical evaluation and not only to be based on laboratory test especially that some 70% patients with positive test results by PCR don’t have any symptoms.
Trending Articles
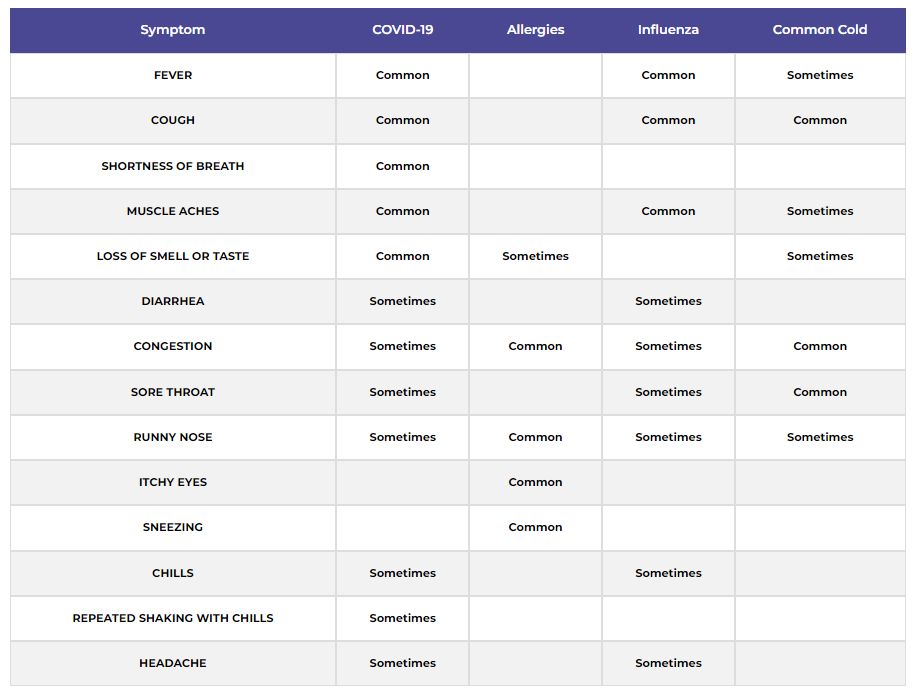
COVID-19 SYMPTOMS
Symptoms may vary from person to person and may range from mild to severe. Symptoms usually occur from 2-14 days after exposure. If you have a cough with fever or shortness of breath, we ask that you call our office BEFORE making an appointment.
Data Source: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html
Chart provided by the American Academy of Allergy Asthma & Immunology. For more information visit, aaaai.org.
Last Updated: January 4th, 2021.
For more information visit the Center for Disease Control at
http://www.cdc.gov or the American Academy of Allergy Asthma & Immunology at http://www.aaaai.org